
Abstract
Our experiences studying exemplar primary care practices, and our work assisting other practices to become more patient centered, led to a formulation of the essential elements of primary care, which we call the 10 building blocks of high-performing primary care. The building blocks include 4 foundational elements—engaged leadership, data-driven improvement, empanelment, and team-based care—that assist the implementation of the other 6 building blocks—patient-team partnership, population management, continuity of care, prompt access to care, comprehensiveness and care coordination, and a template of the future. The building blocks, which represent a synthesis of the innovative thinking that is transforming primary care in the United States, are both a description of existing high-performing practices and a model for improvement.
INTRODUCTION
Achieving the triple aim of health reform—better health, improved patient experience, and more affordable costs—is dependent on a foundation of high-performing primary care. To this end, a vigorous movement is underway to re-engineer primary care practices. Both patients and care providers feel uncertain about how this new primary care model looks. Practices could benefit from a roadmap to help navigate the journey from old to new. In this article we describe a conceptual model that guides our work as practice improvement facilitators: the 10 building blocks of high-performing primary care. The model represents the synthesis of our thinking from a decade of observing and experiencing improvement work in primary care.
METHODS
Our development of the building blocks framework was based on case study methods using information from several sources: site visits by the authors and colleagues to 23 highly regarded practices,1,2 our experiences as practice facilitators in more than 25 practices, and a review of existing models and research on primary care improvement. Seven site visits were performed by the authors; for the others, the authors reviewed site visit reports, looking for descriptions of building block implementation.
Practices were selected for site visits on the basis of being known as innovators and having a reputation for high performance in 1 or more of the triple aims. The 23 practices included 8 hospital-based clinics, 7 integrated delivery system sites, 6 federally qualified health centers, and 2 independent private practices. Seven of the 23 practices had 5 or fewer physicians.2 Most of the 25 practices for which the authors have worked as practice facilitators are federally qualified health centers.
From these case studies and coaching experiences, we used an iterative process to identify common attributes of high-performing primary care. By comparing and discussing field notes, we discerned a set of elements—building blocks—that occurred with regularity among well-functioning practices. We cross-referenced emerging building block concepts with themes articulated in other published frameworks to look for shared elements. These frameworks included the Joint Principles of the Patient-Centered Medical Home (PCMH),3 various medical home recognition standards, the Change Concepts for Practice Transformation,4 University of Utah’s Care by Design,5 and published research on practice transformation.6,7 We also vetted the model with practices during our work in the field and refined the model in response to their feedback.
Our development of the building block model was prompted by our recognition of some important limitations of existing frameworks for understanding the key attributes of high-performing primary care.
Starfield’s 4 Pillars of Primary Care
In 1992 Barbara Starfield articulated the 4 pillars of primary care practice: first-contact care, continuity of care, comprehensive care, and coordination of care.8,9 These pillars were the foundation for all future elaborations of key primary care attributes. In 2007, 4 primary care professional societies coalesced around a vision for primary care—the Joint Principles of the Patient-Centered Medical Home.3 Although the Starfield pillars and Joint Principles describe the essential functions of primary care, they do not offer specific guidance on operationalizing these functions.
Patient-Centered Medical Home Recognition Standards
The publication of the Joint Principles stimulated efforts to define the PCMH in more detail. Propelling this effort was the willingness of some payers to consider enhanced payments to practices meeting certain qualifications. In 2008 (modified in 2011) the National Committee on Quality Assurance (NCQA) unveiled a PCMH recognition process with specific requirements.10 The Joint Commission and URAC have developed their own recognition programs.11
Practices find PCMH standards useful for targeting their improvement efforts; however, the PCMH recognition process has come under criticism. Practices may receive recognition without making fundamental change. Some believe that NCQA requirements are excessively prescriptive, using a checklist approach that may not be responsive to the needs of practices and patients.12 A study of 30 Los Angeles community health centers found no association between NCQA medical home scores and the quality of diabetes care.13 Initiatives assisting practices to transform suggest that the process is long and complex.6
Research on Practice Transformation
Researchers studying primary care improvement have identified several facilitators and barriers to change.6,14,15 These findings, however, have not been formally codified into a set of core capabilities of high-performing primary care that can guide self-improvement work.
THE 10 BUILDING BLOCKS
The 10 building blocks of primary care embrace the Starfield 4 pillars, elements of the Joint Principles and PCMH recognition standards, and other core components (Figure 1). Although the practices we have studied and coached vary the order of implementing the building blocks, many have first established the 4 foundational building blocks of engaged leadership, data-driven improvement, empanelment, and team-based care before achieving success in the higher order blocks. For example, the Starfield essential primary care functions of access, continuity, comprehensiveness, and coordination perch near the top of the building blocks hierarchy; first-tier blocks often support achievement of these functions.
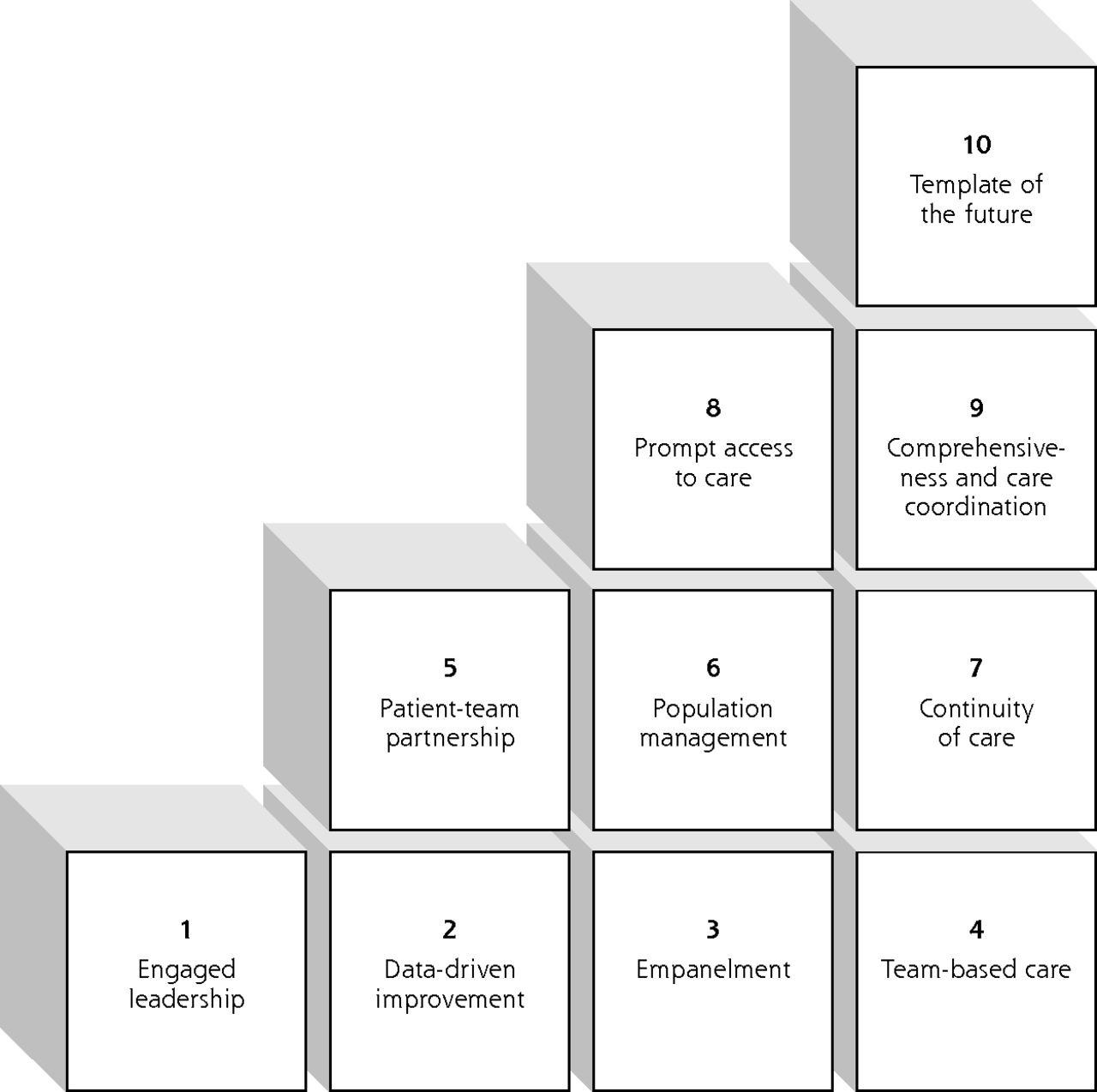
Ten Building blocks of high-performing primary care.
Block 1: Engaged Leadership, Creating a Practice-wide Vision With Concrete Goals and Objectives
High-performing practices have leaders fully engaged in the process of change. Even natural leaders learn the science of how to facilitate organizational transformation. High-performing practices have leadership at all levels of the organization; medical assistants, receptionists, clinicians, and other staff take on the mantle of changing how they and their colleagues do their work. Some engage patients in leadership roles, calling upon them as experts in the health care experience to identify priorities for improvement. Leaders create concrete, measurable goals and objectives, such as, the percentage of our patients with diabetes who have glycated hemoglobin (HbA1c) levels greater than 9% will decrease from 20% to 10% by December 31, 2013.
Block 2: Data Driven Improvement Using Computer-Based Technology
Monitoring progress toward objectives requires the second building block: data systems that track clinical (eg, cancer screening and diabetes management), operational (continuity of care and access), and patients’ experience metrics. Performance measures are often drilled down to each clinician and care team and are regularly shared with the entire staff to stimulate and evaluate improvement. Data charts may be displayed in prominent locations on the walls of the practice, and performance data are discussed in team meetings.
Block 3: Empanelment
Empanelment means linking each patient to a care team and a primary care clinician.16 Even though empanelment requires constant monitoring,16 many practices have viewed it as foundational. Empanelment is the basis for the therapeutic relationship that is essential for good primary care. To improve continuity (block 7) and establish a patient-team partnership (block 5), it is desirable that patients and care teams know each other. Empanelment interacts closely with team formation because teams assume responsibility for their patient panel.
Empanelment enables the practice to calculate adjusted panel size, which determines whether each clinician and team has a reasonable balance between patients’ demand for care and the capacity to provide that care.17 Demand exceeding capacity impedes prompt access to care (block 8). Empanelment allows practices to adjust the workload among clinicians and teams.
Defined panels provide a denominator for performance measures (block 2). How does a clinician know the percentage of her diabetes patients with HbA1c levels greater than 9%? First she needs to know the denominator: how many patients with diabetes are in her panel. Empanelment is also essential for identifying the patient population and stratifying by need for population management (block 6).
Block 4: Team-Based Care
High-performing practices view teams as a necessity for the survival of adult primary care. Clinicians without teams caring for a panel of 2,500 patients would spend 17.4 hours per day providing recommended acute, chronic, and preventive care.18 Yet panel size will inevitably grow as the shortage of adult primary care clinicians worsens.19 Many exemplar practices have created teams with well-trained nonclinicians who add primary care capacity.1 Building teams that add capacity is called “sharing the care.”20
A problem with large teams is that patients may not identify 1 or 2 team members who know them well. To address this issue, high-performing practices generally organize their teams around teamlets—a stable pairing of a clinician and clinical assistant(s) who work together every day and share responsibility for the health of their panel.1 Some practices have increased productivity or panel size by having 2 or 3 clinical assistants for each clinician.1,21,22 Often a larger team—perhaps a registered nurse, social worker, pharmacist, and behaviorist—supports several teamlets.
Some high-performing practices introduce side-by-side colocation of clinicians and nonclinician staff in common work areas (called pods), agree on ground rules that establish a respectful culture, perform daily huddles, and write standing orders empowering nonclinician staff to share the care. Practices may increase their panel size by assigning a subpanel of patients with uncomplicated chronic conditions to nurses or pharmacists who manage the chronic condition using standing orders.1,23,24
Block 5: The Patient-Team Partnership
An effective partnership recognizes the expertise that patients bring to the medical encounter, as well as the evidence base and medical judgment of the clinician and team. Patients are not told what to do but are engaged in shared decision making that respects their personal goals. For patients with chronic conditions, health coaching (see block 6) provides a framework for self-management support.25,26
Block 6: Population Management
High-performing practices stratify the needs of their patient panels and design team roles to match those needs. Three population-based functions provide major opportunities for sharing the care: panel management, health coaching, and complex care management. Panel management involves a staff member, usually a medical assistant or nurse, periodically checking the practice registry to identify patients who are due for routine services (eg, mammograms, colorectal cancer screening, and HbA1c or low-density lipoprotein cholesterol laboratory work). Alternatively, the panel manager can check the health maintenance screen on the electronic medical record before a huddle or medical visit to look for care gaps for these services.27 Standing orders enable panel managers to address care gaps without involving the clinician. In some practices, most routine care is completed before the clinician enters the examination room, so that visits can focus on patients’ concerns, issues requiring the clinician’s level of expertise, treatment options, and shared care plans.
For patients with chronic conditions, health coaching entails assessing patients’ knowledge and motivation, providing information and skills, and engaging patients in behavior-changing action plans known to improve outcomes.25,28 Diabetes patients working with health coaches, whether medical assistants or other patients with diabetes, may have better outcomes than patients without health coaches.29,30 When medical assistants, nurses, health educators, or pharmacists act as health coaches, they usually are given protected time to assume this time-consuming function.
Complex care management has emerged as a way to address patients’ needs that are medically and psychosocially complex, as well as patients who are high utilizers of expensive services. Teams headed by registered nurses or social workers have been shown to improve care and reduce costs for patients needing complex care management.31 Health coaching and complex care management take considerable time, and small practices can benefit from outside organizations assisting them with these functions.32,33
Block 7: Continuity of Care
Continuity of care is associated with improved preventive and chronic care, greater patient and clinician experience, and lower costs.34 To achieve continuity requires empanelment (block 3), which links each patient to a clinician and team. High-performing practices measure continuity for each clinician and achieve continuity goals of 75% to 85%. Reaching these goals requires the front desk staff to encourage patients to see the clinician to whom they are empaneled.1
Block 8: Prompt Access to Care
Access is closely linked to patient satisfaction and is a prominent objective for many practices. Though the science of access is well-developed,35 practices frequently fail in their efforts to reduce patient waiting.36 Our experience has been that practices are more successful at improving access in a sustainable way when they first measure and control panel size (block 3) and build capacity-enhancing teams (block 4). Access and continuity may be in tension if patients prefer to see any clinician today than their own clinician next week. High-performing practices allow patients to decide which takes priority.
Block 9: Comprehensiveness and Care Coordination
One of Starfield’s 4 pillars is comprehensiveness—the capacity of a practice to provide most of what patients need. Another pillar—care coordination—is the responsibility of primary care to arrange for services that primary care is unable to provide.37 When a patient’s needs go beyond primary care practice’s level of comprehensiveness, care coordination is required with the other members of the medical neighborhood, such as hospitals, pharmacies, and specialists. In high-performing systems, clinicians automatically learn when their patients have been discharged from the hospital, and specialist referrals are used to their greatest capacity because diagnostic studies are secured in advance by the primary care clinician.38 Improving care coordination requires teams because busy clinicians lack the time required to coordinate care for every patient with every health care institution. High-performing practices often include a care coordinator or referral coordinator whose sole responsibility is care coordination.
Block 10: Template of the Future
The crown of the building blocks is the template of the future.39 Few practices have achieved this ultimate goal: a daily schedule that does not rely on the 15-minute in-person clinician visit but offers patients a variety of e-visits, telephone encounters, group appointments, and visits with other team members. Clinicians would have fewer and longer in-person visits and protected time for e-visits and telephone visits. With a team empowered to share the care, clinicians would be able to assume a new role—clinical leader and mentor of the team.
Full implementation of this future template requires payment reform that does not reward primary care simply for in-person clinician visits. Some practices are receiving non–visit-based care coordination and pay-for-performance dollars in addition to fee-for-service reimbursement, payments that begin to support new modes of patient encounters. More transformative is to eliminate fee-for-service payments altogether and pay for primary care on a risk-adjusted comprehensive fee per patient with adjustments for quality and patient experience. If primary care practices can reduce unnecessary emergency department and hospital costs for their patients, these practices could also receive a portion of the cost savings.40
DISCUSSION
The 10 building blocks provide a practical conceptual model that can help practices in the journey toward becoming high-performing patient-centered medical homes. This model was derived from our observations of highly regarded primary care practices and from our engagement with other clinics on the journey of transformation. The building blocks focus on design elements largely under the control of the practice or practice organization. Clearly, external reforms are needed to support the building blocks—principally a reformed payment model.
Our development of the building blocks has important methodological limitations. Small, independent private practices are underrepresented in the case studies and practices we have coached. In 2008, 47% of practices included 5 or fewer physicians,41 although there is an accelerating trend toward consolidation.42,43 The building blocks model needs further refinement to be useful for small private practices. Nutting et al, summarizing their studies of small practices, concluded that there is “a set of characteristics found in many small primary care practices that are substantially unlike those in large integrated systems or federally qualified health centers.” These researchers, however, also posited several key attributes needed for small practices to succeed in advanced primary care models that align with the building blocks model: “rethinking the mission and strategies of the practice [block 1]; embracing the need for a meaningful care team approach [block 4]; and adopting a proactive, population-based approach to care [block 6].”14
We did not empirically test whether sequentially focusing improvement work using the building blocks as ordered from 1 to 10 is superior to other pathways of building block implementation. Although our observations and experiences have led us to suggest a degree of hierarchy in the building blocks, with some blocks being enablers of others, we acknowledge that there no single right way of moving forward on practice improvement.
Our work on the building blocks model has not yet included research to systematically and quantitatively test whether practices that have more fully implemented the 10 building blocks perform better on triple aim measures than practices implementing fewer building blocks. An extant evidence base exists, however, for most of the individual building blocks, demonstrating a favorable association with outcomes. For example, research has documented the salutary effects of continuity of care,34 a population-oriented approach to chronic care,44 teamwork,45 and care coordination.37 The foundational building blocks of engaged leadership and data-driven improvement are well-established precepts of quality improvement. Some evaluations, using other models and tools for assessing PCMH capabilities, overlap with many building block components and have found an association between a higher level of these attributes and better clinical performance.46,47
To facilitate and evaluate improvement with the practices we coach, we have piloted a building block assessment (Supplemental Appendix), adapted from an instrument developed by the MacColl Center for Health Care Innovation. Although further research is needed to rigorously validate this instrument, we have found it useful as a self-assessment tool.
The 10 building blocks synthesize the innovative thinking that is inspiring the national movement for high-performing primary care. Even though the building blocks are not a universal roadmap, they can provide an overview that assists practices to transform.
Footnotes
-
Conflicts of interest: authors report none.
-
Previous presentations: Limited portions of this article were presented at University of California San Francisco, May 2012; Colorado Academy of Family Physicians, April 2013; University of Rochester School of Medicine, May 2013; and Kansas University Medical School, May 2013.
-
Supplementary materials: Available at http://www.AnnFamMed.org/content/12/2/166/suppl/DC1/
- Received for publication May 9, 2013.
- Revision received August 22, 2013.
- Accepted for publication September 12, 2013.
- © 2014 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Successful Implementation of Integrated Behavioral Health
- Vulnerable older peoples views on proactive care planning: a qualitative interview study in primary care
- Evaluation of a Program Designed to Support Implementation of Prescribing Medication for Treatment of Opioid Use Disorder in Primary Care Practices
- Global health inequity and primary care
- The role of the primary healthcare research community in addressing the social and structural determinants of health: a call to action from NAPCRG 2023
- Toward a universal definition of provider-patient attachment in primary care
- The Shoeshine Stand and the Renaissance of Primary Care
- Public experiences and perspectives of primary care in Canada: results from a cross-sectional survey
- Effects of Academic Detailing, Panel Management and Mailed Multi-Target Stool-DNA Testing on Colorectal Cancer Screening
- High-Performing Teamlets in Primary Care: A Qualitative Comparative Analysis
- Ensuring Community Is at the Table in Family and Community Medicine Research: Highlighting Dr. Kevin Grumbachs Speech as Recipient of the 2022 NAPCRG Wood Award
- Impact of primary care usual provider type and provider interdependence on outcomes for patients with diabetes: a cohort study
- Factors influencing family physician engagement in practice-based quality improvement: Qualitative study
- Lessons from the implementation of a trauma center-based program to support primary care providers in managing opioids and pain after trauma hospitalization
- High-performing primary care: reinvigorating general practice as a learning health system
- Organizational Factors Associated with Guideline Concordance of Chronic Disease Care and Management Practices
- Measuring the Value Functions of Primary Care: Physician-Level Continuity of Care Quality Measure
- Study protocol: primary healthcare transformation through patient-centred medical homes--improving access, relational care and outcomes in an urban Aboriginal and Torres Strait Islander population, a mixed methods prospective cohort study
- Organizational Factors Associated with Guideline Concordance of Chronic Disease Care and Management Practices
- "Beyond Just a Supplement": Administrators' Visions for the Future of Virtual Primary Care Services
- Patient-centred care delivered by general practitioners: a qualitative investigation of the experiences and perceptions of patients and providers
- Patient characteristics associated with enrolment under voluntary programs implemented within fee-for-service systems in British Columbia and Quebec: a cross-sectional study
- Essential Indicators of Quality in Primary Care Settings: An Evidence-Based, Structured, Expert Approach
- 'Trying to fly the plane while we were building it. Applying a learning health systems approach to evaluate early-stage barriers and facilitators to implementing primary care transformation: a qualitative study
- Impact of Team-Based Care on Emergency Department Use
- Team-based care Evaluation and Adoption Model (TEAM) Framework: Supporting the comprehensive evaluation of primary care transformation over time
- Modes de remuneration alternatifs: Une voie a suivre
- Alternative payment models: A path forward
- Using positive deviance to improve timely access in primary care
- Why does continuity of care with family doctors matter?: Review and qualitative synthesis of patient and physician perspectives
- Intensity of outpatient physician care in the last year of life: a population-based retrospective descriptive study
- Survey protocol for exploring video and phone use in Aotearoa New Zealand general practice: considerations for future telehealth
- Strategies and Factors Associated With Top Performance in Primary Care for Diabetes: Insights From a Mixed Methods Study
- How Comprehensive Medication Management Contributes to Foundational Elements of Primary Care
- Interdisciplinary Primary Care Team Expertise and Diabetes Care Management
- Engagement of Small to Medium-Sized Primary Care Practices in Quality Improvement Efforts
- A Taxonomy for External Support for Practice Transformation
- Care Practices to Promote Patient Engagement in VA Primary Care: Factors Associated With High Performance
- Practice Transformation Support and Patient Engagement to Improve Cardiovascular Care: From EvidenceNOW Southwest (ENSW)
- The Built Environment for Professionalism
- Evaluation of a learning collaborative to advance team-based care in Federally Qualified Health Centers
- Improving access in a VA primary care clinic using an innovative Panel Retention Tool: a quality improvement report
- Association of physician payment model and team-based care with timely access in primary care: a population-based cross-sectional study
- Patient and primary care physician characteristics associated with billing incentives for chronic diseases in British Columbia: a retrospective cohort study
- Complex programme evaluation of a 'new care model vanguard: a shared commitment to quality improvement in an integrated health and care context
- Evaluating the implementation of collaborative teams in community family practice using the Primary Care Assessment Tool
- Features of U.S. Primary Care Physicians and Their Practices Associated with Advance Care Planning Conversations
- Attachment to primary care and team-based primary care: Retrospective cohort study of people who experienced imprisonment in Ontario
- Primary health care performance: a scoping review of the current state of measurement in Africa
- HIGH-PERFORMING PRIMARY CARE RESIDENCY CLINICS: A COLLABORATION
- A Randomized Trial of External Practice Support to Improve Cardiovascular Risk Factors in Primary Care
- Connecting People With Multimorbidity to Interprofessional Teams Using Telemedicine
- A Longitudinal Study of Trends in Burnout During Primary Care Transformation
- Primary Care Practices' Implementation of Patient-Team Partnership: Findings from EvidenceNOW Southwest
- Engaging primary care physicians in care coordination for patients with complex medical conditions
- Burnout and Health Care Workforce Turnover
- Shared vision for primary care delivery and research in Canada and the United States: Highlights from the cross-border symposium
- Recruiting Primary Care Practices for Research: Reflections and Reminders
- Practice-based Research Network (PBRN) Engagement: 20+ Years and Counting
- Improving the quality of health care in Canada
- How health care may modify the effects of illness determinants on population outcomes: the Leicester SEARCH conceptual framework for primary care
- The influence of patient-clinician ethnocultural and language concordance on continuity and quality of care: a cross-sectional analysis
- Alternative Payment Models and Team-Based Care
- Processes that influence the evolution of family health teams
- Roles and Functions of Community Health Workers in Primary Care
- Association of the Social Determinants of Health With Quality of Primary Care
- Identification of physicians providing comprehensive primary care in Ontario: a retrospective analysis using linked administrative data
- The Patient-Centered Medical Home (PCMH) Framing Typology for Understanding the Structure, Function, and Outcomes of PCMHs
- Team-based primary care with integrated mental health is associated with higher quality of care, lower usage and lower payments received by the delivery system
- Building a Sustainable Primary Care Workforce: Where Do We Go from Here?
- Increased Health Information Technology Adoption and Use Among Small Primary Care Physician Practices Over Time: A National Cohort Study
- Association Between Physician Teamwork and Health System Outcomes After Coronary Artery Bypass Grafting
- Perspectives of Primary Care Providers Toward Palliative Care for Their Patients
- Care Coordination and Population Management Services Are More Prevalent in Large Practices and Patient-centered Medical Homes
- Integrating Social And Medical Data To Improve Population Health: Opportunities And Barriers
- "A Paradox Persists When the Paradigm Is Wrong": Pisacano Scholars' Reflections from the Inaugural Starfield Summit
- Toward evidence-based policy
- A Primary Care Panel Size of 2500 Is neither Accurate nor Reasonable
- Family Medicine Panel Size with Care Teams: Impact on Quality
- Processes of patient-centred care in Family Health Teams: a qualitative study
- Perspectives in Primary Care: A Conceptual Framework and Path for Integrating Social Determinants of Health Into Primary Care Practice
- Achieving Value in Primary Care: The Primary Care Value Model
- Large Independent Primary Care Medical Groups
- Teamlets in Primary Care: Enhancing the Patient and Clinician Experience
- Longitudinal evaluation of physician payment reform and team-based care for chronic disease management and prevention
- Perspectives in Primary Care: The Foundational Urgent Importance of a Shared Primary Care Data Model
- Patient Empanelment: The Importance of Understanding Who Is at Home in the Medical Home
- Only One Third of Family Physicians Can Estimate Their Patient Panel Size
- Health Is Primary: Family Medicine for America's Health
- On-the-Ground Wisdom About Care Integration